Encourage abstinence-only treatment.
Quick fixes rarely solve complex, multi-faceted problems.
Lots of news lately on Medication Assisted Treatment (see HHS story here)
Here’s information to help you better understand what is being talked about:
Medication Assisted Treatment (MAT)
What is MAT?
- Anti-craving medications which are non-addictive / non-psychoactive substances such as Naltrexone and Acamprosate. These are not drugs that can be abused to get high.
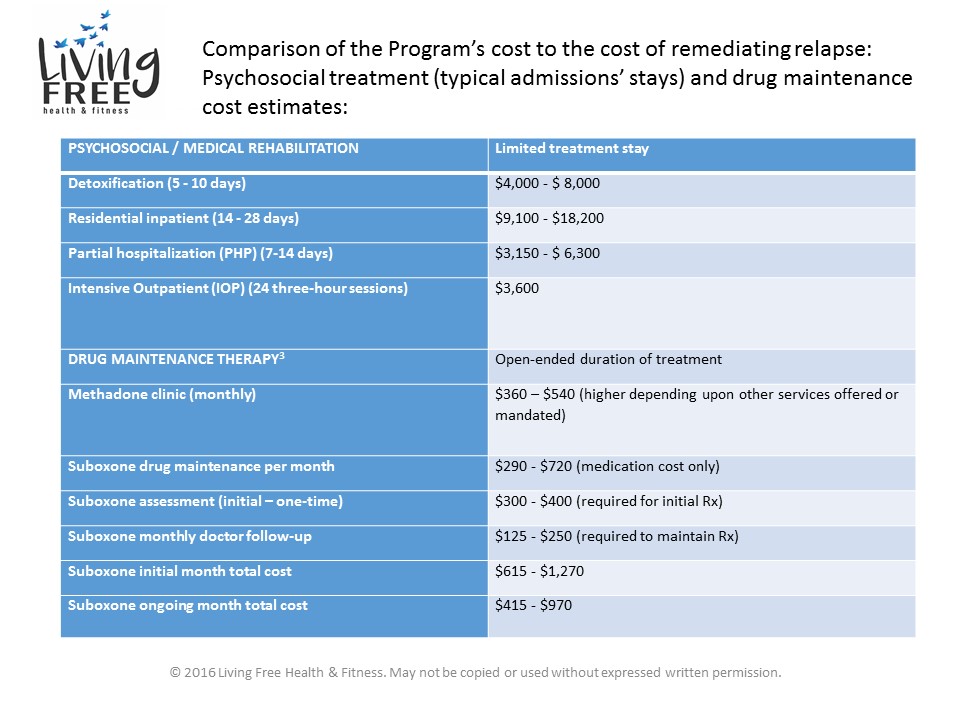
- Opioid replacement drugs such as buprenorphine-based drugs like Subutex and Suboxone, and Methadone. These drugs are used for both detoxification and for “maintenance”. These medications are psychoactive and can be abused to get high.
To the layman, the anti-craving medications probably make sense. Take a pill or injection to cut cravings for certain drugs of abuse (including opiates and alcohol), and diminish or block the “high” effect, in the event of relapse.
But what about the “maintenance” drugs? Why on Earth would you replace one opiate with another as an intervention? It seems to defy logic. The theory behind such replacement is “harm reduction”. Drugs like Methadone and Buprenorphine don’t involve needles, overdoses on these substances alone are atypical, the product is a quality-controlled/dosed product, are highly regulated and are prescribed by providers with special licensing and training. Hooked on Suboxone is thought of as better than hooked on heroin. Harm reduction.
And that make sense. To a point.
In spite of evidence indicating medical benefits of maintenance drugs to some chronically relapsing individuals, this method of treatment has significant drawbacks:
- Individuals are frequently kept on these psychoactive substances for months or years, depriving them of engaging in independent lives and making them subject to long, arduous and expensive detoxification to stop these medications (Much worse than detox from heroin or prescription pills!);
- That grueling detoxification can increase the potential of relapse onto street drugs;
- The high cost of treatment of approximately $320 – $720 month — excluding assessment and doctor follow-up;
- The risk of over-prescribing in response to community concerns to “do something” to stop the current opioid epidemic.
So here is our take on this:
First of all, the individual is STILL HOOKED on an opioid substance! Being dependent on a replacement drug is, well, DEPENDENCE! Remember, abstinence is liberty.
Psychoactive substances affect the ability to manage impulses, delay gratification, schedule and plan, and to adequately assess potential consequences. If the prescription runs out there is strong compulsion to get more. Many people use more than prescribed and seek higher doses from their prescribers. The drug is sold and abused just like any other street or controlled prescription substance.
Opiates, and psychoactive substances in general, numb us to our feelings! If we are under the influence of any mood and personality altering drug, just how much “work” can be made on effecting the sorts of cognitive, behavioral, and emotional changes necessary to living a lifetime of staying stopped? One of the biggest relapse factors in recovering persons is lack of insight and ability in dealing with emotions and conflicts.
Bottom line? Avoid maintenance therapy. It offers false promise. It kicks the can down the road. Anecdotal evidence from those having experienced detox from heroin/pills and detox from buprenorphine or methadone describe exponentially worse detox experiences as measured by duration of detoxification and the severity of both physical and emotional acute and post-acute withdrawal symptoms.